


Ask a compliance officer at a mid-size hospital system what takes up most of their week, and the honest answer is rarely the training content itself. It's the reconciliation work: confirming which nurses are current on their licenses, chasing down outstanding HIPAA refreshers before a deadline, pulling together evidence for an upcoming Joint Commission survey from three different spreadsheets that don't quite agree with each other.
Healthcare compliance training is structurally harder to manage than compliance training in most other industries, not because the content is more complicated, but because the obligations stack. A single organization is typically managing HIPAA privacy and security training, OSHA workplace safety requirements, Joint Commission accreditation standards, state-specific licensure renewal for multiple clinical professions, and a layer of internal policy training that applies to everyone regardless of role. Each of these has its own renewal cadence, its own audience, and its own audit expectations, and most healthcare organizations are tracking all of it through some combination of spreadsheets, email reminders, and institutional memory.
That combination works, more or less, until it doesn't. A renewal gets missed because the spreadsheet owner was out sick the week the alert should have gone out. An auditor asks for evidence of infection control training going back eighteen months, and producing it takes three days of cross-referencing instead of three minutes. A new hire starts working clinical shifts before their background-dependent training is actually verified as complete. None of these failures happened because anyone was careless. They happen because the underlying system was never built to hold this much complexity without manual intervention at every step.
The cost of getting this wrong is not abstract. A missed license renewal can mean a clinician working without legal authority to practice, exposing the organization to liability and putting patient safety at direct risk. A weak audit trail during a Joint Commission survey or a state inspection can trigger findings that take months to remediate and can affect accreditation status. And the administrative cost compounds quietly: every hour a compliance officer spends reconstructing records by hand is an hour not spent on the work that actually reduces risk, identifying genuine gaps before they become findings, rather than documenting gaps after the fact.
This piece looks at what actually simplifies healthcare compliance management, not by adding more policies or more oversight, but by changing the structure underneath the training and tracking itself, so the system absorbs complexity that currently falls on a person's shoulders every renewal cycle.
What Is the Best Way to Simplify Healthcare Compliance Training?
The most effective way to simplify healthcare compliance training is to stop treating it as one undifferentiated program and instead structure it around three changes: tiering compliance categories by regulatory and patient-safety weight rather than tracking everything in a single mandatory-training bucket, automating certification and license tracking with renewal alerts that escalate as expiry approaches, and centralizing policy acknowledgment and audit evidence in one system rather than scattered spreadsheets and email threads. Organizations that simplify successfully are not the ones with the least training content. They are the ones whose underlying tracking infrastructure does the reconciliation work automatically instead of requiring a person to do it manually before every audit or every renewal deadline.
Why Healthcare Compliance Feels Harder Than It Should
Three structural patterns explain why compliance management in healthcare consumes so much more administrative time than the actual training content would suggest.
The first is regulatory stacking. Most industries manage one or two major compliance frameworks. A healthcare organization is typically managing HIPAA, OSHA, Joint Commission, or equivalent accreditation standards, state licensure boards for multiple professions, and CMS conditions of participation, where applicable, often simultaneously and often with overlapping but not identical requirements. A single staff member, a nurse with prescriptive authority, for example, may sit inside five or six of these obligations at once.
The second is the clinical and non-clinical split. A hospital employs licensed clinicians whose compliance requirements include continuing education and competency assessment, alongside non-clinical staff in HR, IT, and facilities, whose compliance needs look like a fairly standard corporate program. Treating both populations identically either over-burdens non-clinical staff with irrelevant clinical content or, more dangerously, under-tracks the credential-specific requirements that actually carry legal weight for clinical roles.
The third is manual reconciliation as the default operating model. When certification status, training completion, and policy acknowledgment live in separate systems, or in spreadsheets maintained by different departments, every audit, every license renewal, and every new-hire onboarding becomes a small reconciliation project. This is the pattern most responsible for the administrative burden compliance teams describe, not the volume of training itself, but the manual work of stitching together a complete picture from disconnected sources.
A fourth, less discussed pattern compounds the first three: compliance content in healthcare tends to age faster than the system tracking it. Regulations update, accreditation standards get revised, and a course built two years ago may no longer reflect current guidance, even though the completion record still shows green. Keeping content current is a separate problem from tracking completion, but the two get conflated often enough that organizations mistake a high completion rate for genuine, current compliance.
Healthcare Regulatory Frameworks Compliance Training Needs to Account For
A healthcare compliance program typically needs to track training and documentation against several distinct regulatory frameworks at once, each with its own renewal logic and audit expectations.
HIPAA governs patient privacy and data security training, generally required at onboarding and refreshed annually, with documentation requirements around who completed it and when.
OSHA covers workplace safety training relevant to healthcare settings, bloodborne pathogens exposure control, hazard communication, and emergency action plans, among others, with its own recordkeeping expectations separate from clinical compliance.
Joint Commission standards, or equivalent state and CMS accreditation requirements, expect organizations to demonstrate ongoing competency and training across a wide range of categories during a survey, often with specific documentation formats auditors expect to see by category rather than as a single completion percentage.
State licensure boards govern individual professional credentials, nursing licenses, physician licenses, allied health certifications, each with its own renewal cycle, continuing education requirement, and registration verification process specific to that profession and that state.
Internal policy training, covering everything from code of conduct to specific clinical protocols, sits alongside all of the above and typically applies to a broader population than any single regulatory framework.
The practical challenge is not understanding each framework individually. It's that most healthcare organizations need to track an individual employee's status against several of these simultaneously, and a system built around a single generic “mandatory training” category struggles to represent that without losing the category-specific detail an audit actually asks for.
A Risk-Tiered Approach to Compliance Categories
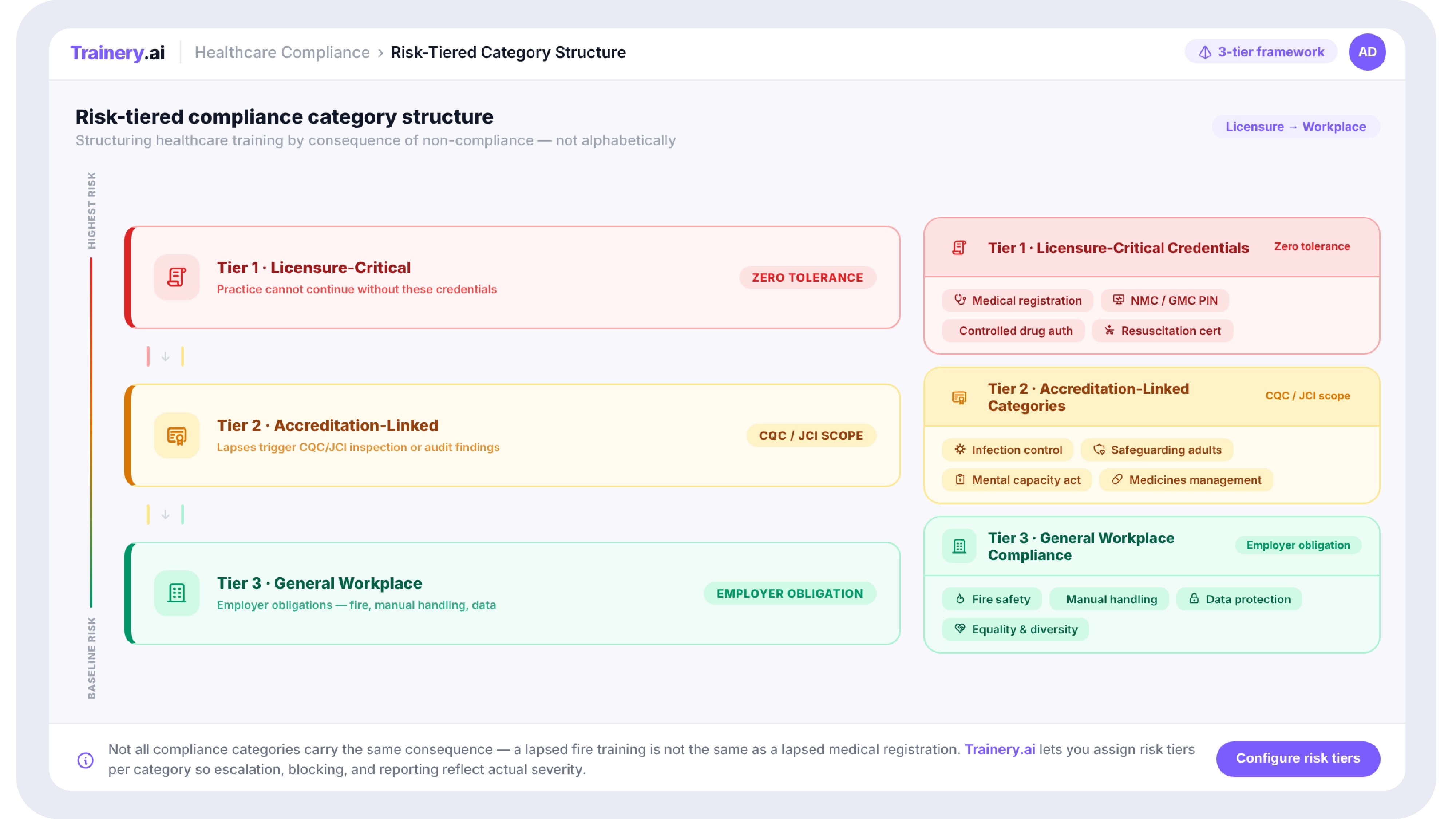
Not every compliance obligation carries the same stakes if it lapses, and treating them identically wastes administrative attention on lower-risk items while under-resourcing the ones that matter most.
A practical risk tier looks roughly like this: at the top, licensure-critical training and credentials, where a lapse has immediate legal and patient-safety consequences, such as a nurse working with an expired license, for example. In the middle, accreditation-linked compliance categories like infection control, safeguarding, and medicines management, where a gap creates real audit exposure and risk, but doesn't necessarily stop someone from working today. At the base, general workplace compliance, data protection refreshers, and anti-harassment training that applies broadly and carries real but more modest consequences if briefly delayed.
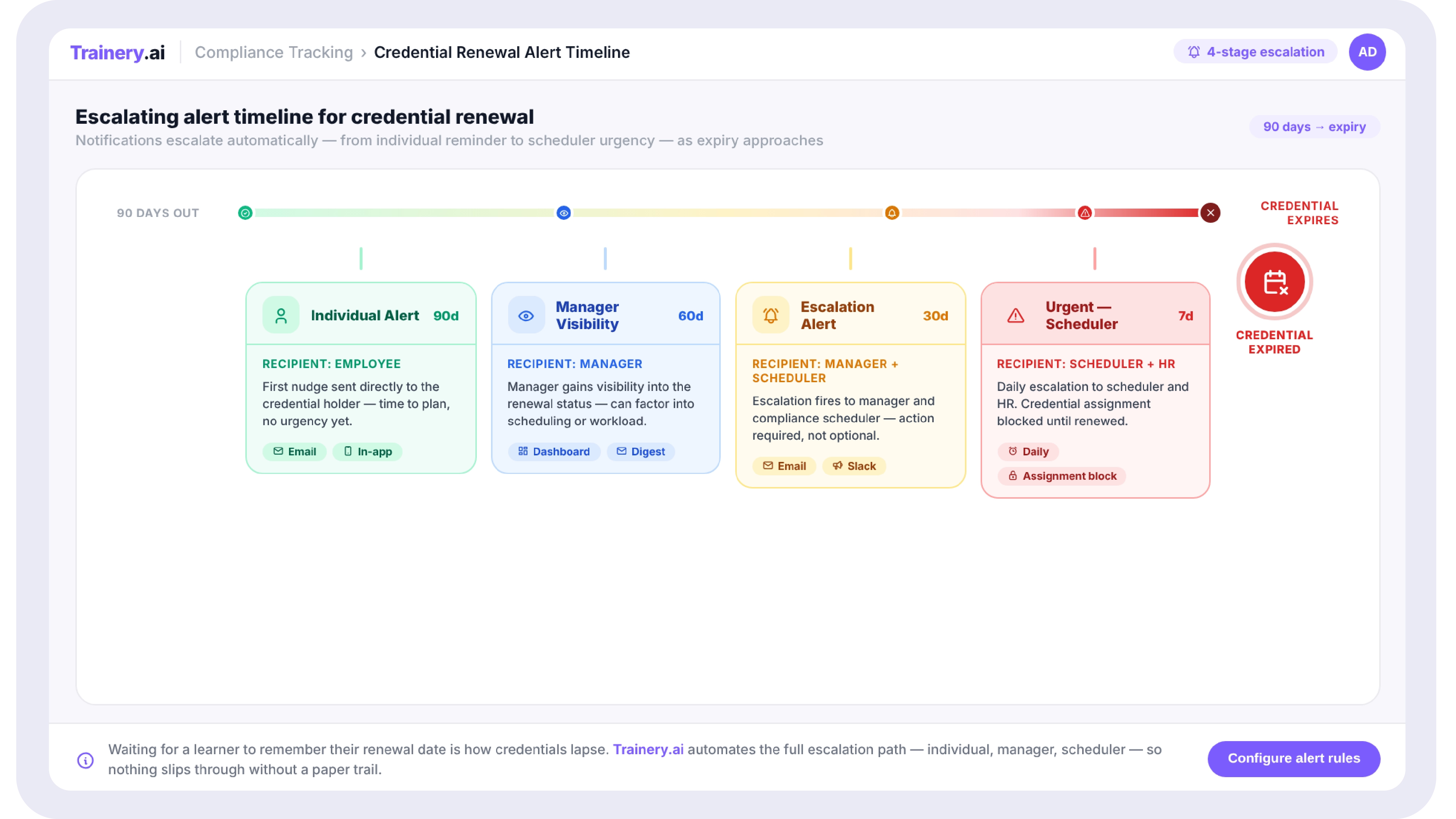
This tiering matters operationally because it changes how alerts, escalation, and reporting should behave. A licensure renewal approaching its deadline should reach a manager and a scheduler, not just sit in an individual's task list, much like the credential tracking escalation logic built specifically for clinical renewal cycles. A general compliance refresher running a few days late is a lower-urgency item that a standard reminder can handle. Most compliance software treats all training identically by default, which means either everything gets escalated, creating alert fatigue, or nothing does, which is how genuinely urgent gaps get missed.
Automating Certification Tracking and License Renewal
Manual certification tracking, typically a spreadsheet with expiry dates and a calendar reminder, breaks down for the same reason most manual systems break down at scale: it depends entirely on someone remembering to check it, and it doesn't differentiate urgency.
An automated approach needs to handle a few things a spreadsheet structurally can't do well. It needs to support multiple renewal models simultaneously, since a single clinician might hold a fixed-expiry license alongside continuing education credits that accumulate over a rolling period rather than expiring on a single date. It needs escalating visibility, so a renewal ninety days out is a planning item visible to the individual, while the same renewal at seven days out reaches a manager or scheduler directly, particularly for roles where a lapsed credential affects scheduling. And it needs to store evidence, not just a status flag, since what most audits and inspections actually ask for is documentation behind a credential's current status, not a green checkmark on a dashboard.
Centralizing Policy Acknowledgment and Audit Trails
A surprising amount of compliance administrative burden comes not from training delivery itself but from policy acknowledgment, confirming that every employee has read and accepted current versions of the code of conduct, HIPAA privacy policies, infection control protocols, and similar documents, and being able to prove it during an audit.
When acknowledgment records live in a separate system from training completion records, or worse, in physically signed forms filed by the department, producing a complete audit trail means manually cross-referencing multiple sources under time pressure. Centralizing acknowledgment tracking alongside training completion and certification status means a single employee record can show, at a glance, every policy version acknowledged, every required course completed, and every credential's current status, with timestamps and evidence attached to each. This is the difference between an audit prep process that takes days of manual compilation and one that takes minutes to generate a report that the system already maintains continuously.
Reducing Administrative Burden Without Reducing Rigor
A common worry when organizations talk about simplifying compliance is that simplification means cutting corners. In practice, the administrative burden and the actual rigor of a compliance program are largely separable. The burden comes from manual reconciliation work: chasing signatures, cross-referencing spreadsheets, and reconstructing records for an audit. The rigor comes from whether the right training happens, whether credentials are genuinely current, and whether evidence exists to support that. Automating the reconciliation work doesn't weaken the rigor. It typically strengthens it, since a system that tracks and escalates consistently catches gaps a manually maintained spreadsheet is more likely to miss, particularly across a large or multi-site organization where no single person has visibility into the whole picture.
What to Look for in Healthcare Compliance Software
A few criteria separate software that genuinely reduces administrative burden from software that simply moves the same manual process onto a screen.
Look for support for multiple renewal cycle types within a single credential record, since fixed-expiry licenses and cumulative continuing-education models need to coexist without forcing one into the other. Look for escalation logic that differentiates by urgency and role, not a single notification tier for every training item, regardless of category. Look for category-specific reporting and analytics that mirror how audits actually ask questions, by compliance category and role rather than a single completion percentage across the whole organization. Look for a clean separation, within one platform, between clinical and non-clinical training paths alongside a shared layer for mandatory training that applies to everyone. And look for integration with the HR and scheduling systems already in use, since a compliance platform that requires duplicate data entry recreates the reconciliation burden it's supposed to remove.
Cost is also a real factor for smaller healthcare providers evaluating options, and it's worth confirming pricing scales reasonably for a clinic or care provider well under enterprise headcount, rather than assuming list pricing built around large hospital systems applies evenly.
Questions to Ask Before Choosing a Compliance Management Platform
- Does the platform support both fixed-expiry and cumulative renewal models within the same credential record?
- How does the system escalate alerts as a deadline approaches, and does that escalation reach managers and schedulers, not just the individual?
- Can compliance reports be generated by category, safeguarding, infection control, medicines management, rather than only as an overall completion percentage?
- What evidence does the system store behind a credential's status, and can that evidence be produced quickly during an audit?
- Does the platform support distinct clinical and non-clinical training paths within one system, alongside shared mandatory training?
- What does implementation and ongoing administration actually require in terms of internal IT or L&D resourcing?
- How does pricing scale for our actual headcount, and does the vendor have experience with organizations of our size specifically?
How This Looks in Practice
Consider a 400-bed regional hospital system managing roughly 3,000 staff across clinical and non-clinical roles. Before consolidating compliance tracking, the L&D team maintained licensure renewal dates in one spreadsheet, OSHA training completions in the LMS's generic reporting, and policy acknowledgment as signed PDF forms scanned into a shared drive by unit. Preparing for an accreditation survey meant roughly two weeks of cross-referencing all three sources by hand, and a licensure gap for a per-diem nurse was missed for several weeks because the spreadsheet's reminder column had not been updated after a format change.
After moving to a system with risk-tiered categories, automated multi-cycle credential tracking, and centralized acknowledgment records, the same audit preparation became a same-day report generation task, and licensure alerts began reaching both the individual and the unit's scheduling lead automatically as renewal dates approached. The underlying training content barely changed. What changed was the infrastructure doing the reconciliation work that previously required a person to do it manually, under time pressure, multiple times a year.
Simplifying healthcare compliance training and certification management isn't about reducing what staff need to know or how often it needs to be verified. It's about removing the manual reconciliation work that currently sits between scattered records and an audit-ready answer. A risk-tiered structure for compliance categories, automated tracking that handles multiple credential renewal models with escalating urgency, and centralized policy acknowledgment and evidence all attack the same underlying problem: too much of the compliance burden in healthcare is administrative friction rather than actual training delivery.
Organizations that simplify successfully build that structure once and let the system carry the reconciliation load going forward, rather than rebuilding the same manual cross-referencing process before every audit and every renewal cycle. The goal is not a smaller compliance program. It is a compliance program where the system, not a person working under deadline pressure, is the one keeping every credential, every policy acknowledgment, and every training record current and provable at any moment, not just in the weeks before a scheduled audit.
.svg)

.svg)
.svg)

